Slider
In Lupane, Catholic sisters bring early childhood education to rural areas

BY MARKO PHIRI
Zimbabwe in recent years has promoted early childhood development, or ECD, making it mandatory for every child to attend such classes before they are accepted into the first grade.
This policy, however, has not been without its challenges, including a shortage of ECD educators and few government-run schools that offer such classes.
That has led to a flourishing of fly-by-night unregistered schools offering preschool lessons.
It has been particularly tough in rural areas, long left behind in the country’s development agenda where children often fail to go to school because of a lack of education facilities and parents’ failure to pay for tuition.
To fill that gap, a diocesan congregation of Catholic sisters has set up two early childhood education schools in Lupane, a poor rural district about170 kilometres north of Bulawayo, Zimbabwe’s second-largest city.
Lupane is a small farming and livestock rearing hamlet with a population of about 200,000 people.
At its centre can be found modern conveniences such as banks, supermarkets, bars, and long-distance buses and truckers going as far as the tourist city of Victoria Falls, 223 kilometres west.
Lupane’s centre is a hive of activity that belies the poor rural incomes found in some villages stretching more than 20 kilometers into the hinterland.
The Servants of Mary the Queen, known by their Latin abbreviation AMR () are a congregation of Indigenous nuns formed in 1956 by Mariannhill missionaries in Bulawayo.
The congregation has about 70 sisters whose apostolate straddles teaching, nursing, communication; general pastoral work; and working with the Bulawayo archdiocese and its rural missions spread across the country’s southwest.
Local government education officials have hailed the early childhood education development programmes run by the sisters as a first in the region with state-of-the-art facilities.
There are two early childhood programs, one in Lupane centre and another at the primary school about two kilometre in Matshiya village.
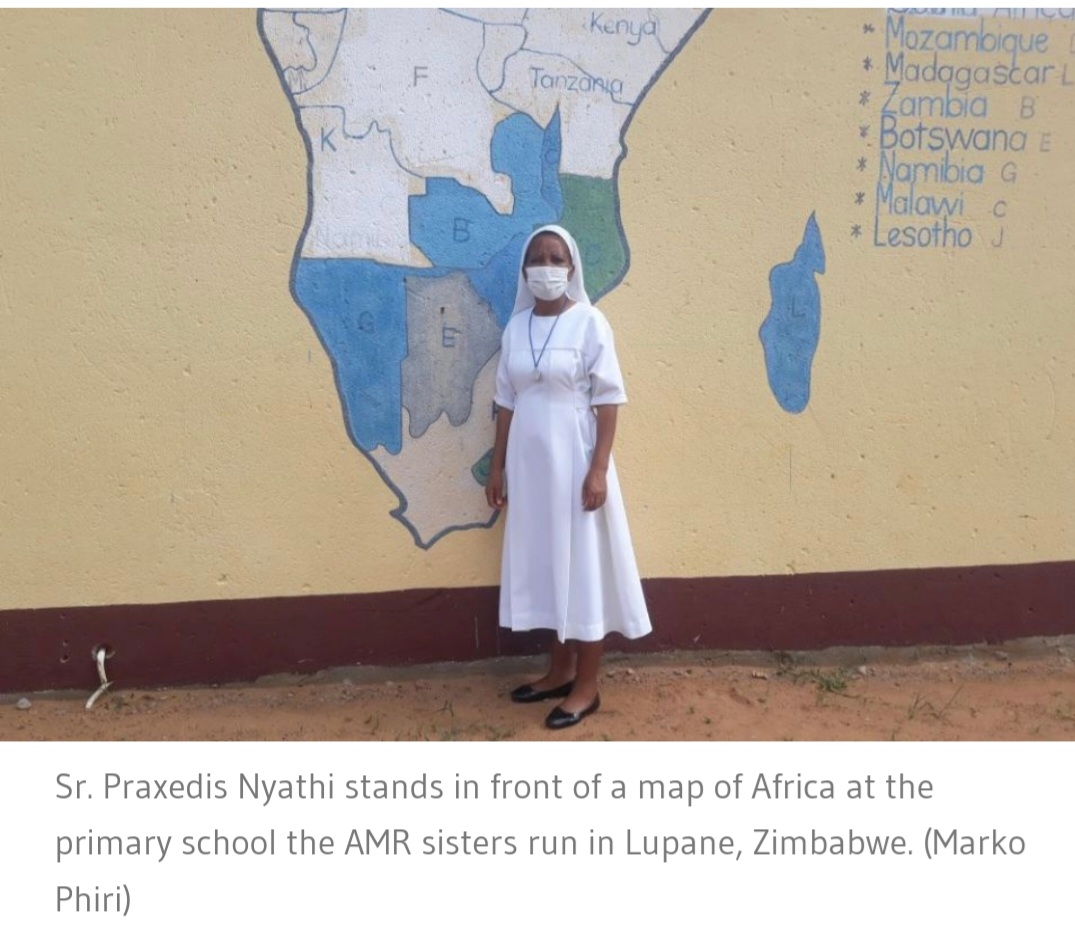
“All children must attend ECD classes. We want to produce well-grounded citizens and the best place to start is in early childhood education,” said Sr. Praxedis Nyathi, who heads the AMR Primary School, from early childhood education to grade seven.
She specialised in early childhood education after having made her final vows as a religious in 1998.
According to Nyathi, the school opened in 2018 in Matshiya village with just over 100 children, from early childhood development classes to grade seven.
That number has since grown to about 500, highlighting the ever-present need to provide education in the country’s rural areas.
At the AMR Primary School, where more classrooms are still under construction, Nyathi says it is challenging to persuade families in rural communities to enroll their children in ECD.
“Some parents try to cut corners and delay enrolling their children and attempt to bring them straight into the first grade.
“But we have made it clear that we will not accept any child who has not attended ECD classes,” Nyathi told GSR.
In Zimbabwe’s rural areas, it is not unusual for parents to choose to send sons to school and keep their daughters at home, believing that the investment in their education will be lost once the girl marries.
Nyathi says the sisters are trying hard to change that attitude.
“We have such cases but ever since we opened the ECD classes, we have been hard at work convincing families to enrol the girl child too.
“We are making small strides but there is still a lot of work to be done,” Nyathi said.
That need to enroll more children at ECD is emphasised by Sr. Midlred Chiriseri, an AMR sister who teaches at the nearby AMR Secondary School, which offers what is known as Form 1 through Form 4 classes for students ages 13 to 17.
Students from the ECD and primary schools run by the congregation feed into the secondary school.
Actually, there is a need to enroll more children at all school levels, Nyathi said.
Parents must be persuaded to bring their children to school, follow up on their schoolwork and be involved in their children’s education.
“It’s a real challenge here in the rural areas where up to 80% of students are non-readers, meaning they cannot articulate themselves as other literate learners of their age would.
“So we have to start them early at ECD to address that,” Chiriseri told GSR.
“What we also need are more religious in Catholic schools if we are to fulfil our mission to instil Catholic values in learners,” Chiriseri said.
The irony is that while some parents remain reluctant to enrol their children, Nyathi says the existing ECD classes are oversubscribed.
“We have a situation where ideally we should have 20 children in one class, but we in fact have up to 42 children, which is a strain on our teachers,” Nyathi said, because the school doesn’t have enough teachers.
The country faces a shortage of teachers , including ECD educators.
Nyathi said that her congregation and other religious congregations send some sisters for teacher training, but it is still the government that deploys them after they graduate, often sending them to government-run schools.

Zimbabwe is celebrated as one of Africa’s most literate countries, and the education ministry says that such gains since the country’s independence in 1980 would not have been possible without the contribution of the Catholic Church.
The country’s education officials say more than 3,000 primary and secondary schools are required to meet Zimbabwe’s education commitments, with rural areas being particularly in need.
Bulawayo Archbishop Alex Thomas has praised the sisters, calling on them to be “educators of life.”
The journey ahead will include ensuring that learners who pass through the AMR schools are well equipped for life as adults, Nyathi said.
She would like to see not just academic excellence but also aptitude in practical subjects that ensure self-reliance in a country where there are few formal jobs.
“Catholic schools should be a place where children find Christ, and by starting them early at ECD, we try to produce self-respecting learners who will make meaningful contributions in their respective communities,” Nyathi said. – Global Sisters Report














-

 Slider3 years ago
Slider3 years agoInnscor launches brewery to produce Nyathi beer
-

 National5 years ago
National5 years agoIn perched rural Matabeleland North, renewable energy is vital
-

 Tourism and Environment4 years ago
Tourism and Environment4 years agoStrive Masiyiwa’s daughter opens luxury Victoria Falls lodge
-

 Special reports4 years ago
Special reports4 years agoTinashe Mugabe’s DNA show’s popularity soars, causes discomfort for some
-

 Opinion4 years ago
Opinion4 years agoA street art mural in Zimbabwe exposes a divided society
-

 National4 years ago
National4 years agoVictoria Falls’ pilot dies in helicopter crash
-

 National3 years ago
National3 years agoCommission of inquiry findings fail to be tabled as Victoria Falls councillors fight
-

 National3 years ago
National3 years agoHwange coal miner fires workers over salary dispute